

The Cheap Peptide Question: What Is Actually Being Purchased?
Last updated: June 2026. Most of the compounds discussed here are prescription or compounded products, and several are not approved by the FDA for the uses men over 40 are chasing. Every clinical and regulatory claim links to a primary source that can be opened and read.
Here is the claim a man makes to himself when he finds a $40 vial of BPC-157 on a research-chemical site instead of paying a clinic’s price: I found the same thing, cheaper. The word doing the damage in that sentence is “same.” Nobody selling that vial has verified that it is the same. And that, more than any moralizing about gray markets, is the actual problem with “cheap” in this category. It isn’t that cheap is wrong. It’s that cheap is being used to answer a question it was never designed to answer.
So set the price question aside for a moment and ask a duller one: what, exactly, is known, what is merely studied, and what is simply unknowable at the point of sale? That distinction, applied check by check, is a more useful filter than sticker price, and it produces a ranking that looks nothing like a “who’s cheapest” list.
An audit, not a price comparison
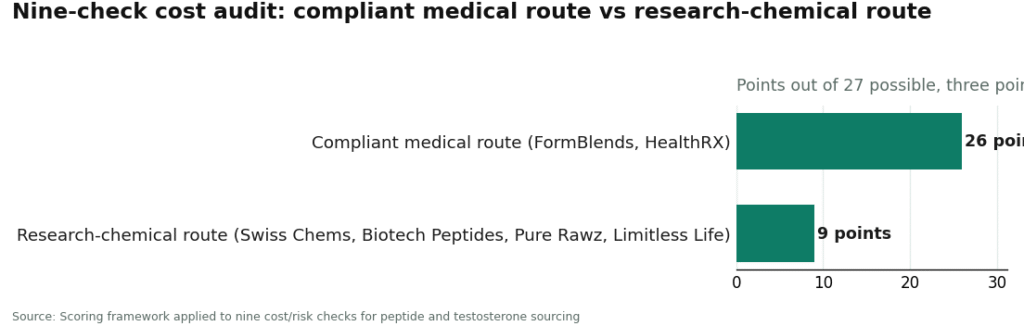
The framework below scores two kinds of sellers against nine questions, three points each, twenty-seven possible. One kind is the compliant medical route: licensed telehealth, physician review, pharmacy dispensing, represented here by FormBlends and HealthRX.com. The other is the research-chemical route, sites selling peptides labeled “for research use only,” represented by Swiss Chems, Biotech Peptides, Pure Rawz, and Limitless Life. They’re graded as a single class because, on every check that isn’t the sticker price itself, they behave identically: no clinician, no independent verification, no follow-up.
What makes this worth doing as an audit rather than a vibe check is that most of the nine questions have a genuine evidence answer, not an opinion. Some things about these compounds are proven. Some are studied but unresolved. Some are, at the point of a research-chemical purchase, structurally unknowable, and that third category is where most of the “savings” actually live.
Check 1: The visible price versus the real one
A research-chemical listing quotes a number. It does not quote the probability that the vial contains what the label says, or the expected cost if it doesn’t. Multiply those in and the “low” price stops being low, it’s just unknown. A supervised route’s higher number is, at least, a number that accounts for identity and dose. An unverified low price loses to a verified higher one whenever the unverified side carries a downside, which here it does.
Compliant route: 3. The price reflects a verified, dispensed product. Research-chemical route: 1. Visible, but not connected to true cost.
Check 2: Does anything actually verify the contents?
This is the check on which the entire argument turns. A certificate of analysis on a research-chemical site is a document the seller decided to post, not an independent finding. It proves the seller can produce a PDF. A licensed compounding pharmacy operates under recognized dispensing standards, which is a different category of assurance entirely, not a nicer version of the same one.
Compliant route: 3. Pharmacy dispensing under recognized standards. Research-chemical route: 1. Seller-issued paperwork only.
Check 3: Does a clinician decide if the compound even fits the buyer?
Some of this risk has nothing to do with dose accuracy and everything to do with the person taking it. TRAVERSE, published in the New England Journal of Medicine in 2023, randomized 5,246 middle-aged and older men with diagnosed hypogonadism and elevated cardiovascular risk to testosterone or placebo. Testosterone did not raise major adverse cardiac events overall, which is the headline finding, but the trial also reported more atrial fibrillation in the testosterone group [6]. That is exactly the kind of finding a price tag cannot resolve. A clinician evaluating fit is the actual safeguard. A checkout page skips the evaluation, full stop.
Compliant route: 3. Review precedes dispensing. Research-chemical route: 0. The buyer self-selects.
Check 4: Does the evidence justify spending anything?
A cheap price on a compound with no human safety data is not a discount, it’s a bet with no odds posted. BPC-157 is the plainest example: a 2025 systematic review in HSS Journal, the Hospital for Special Surgery’s publication, found the literature is almost entirely preclinical, animal and cell studies, with no human clinical safety data and no FDA-approved indication [5]. The growth-hormone-releasing peptides sit on firmer, though still modest, ground. A 1992 study in the Journal of Clinical Endocrinology and Metabolism found GHRH (1-29) reversed the age-related decline in GH and IGF-1 in older men [1]. A 2006 study in the same journal found CJC-1295 raised GH and IGF-1 for days after one dose [3]. “Studied” and “proven for this use in this population” are not the same claim, and a clinician can say so out loud. A vial cannot.
Compliant route: 3. Spend filtered by evidence review. Research-chemical route: 1. The buyer carries the evidence gap alone.
Check 5: Is the saving real, or is it deferred monitoring?
Testosterone requires follow-up precisely because of what TRAVERSE documented [6], and companion medications like HCG or enclomiphene exist to manage its downstream effects. A research-chemical vial ships with none of that. The buyer hasn’t saved the cost of monitoring, he’s postponed it, and postponed costs tend to compound.
Compliant route: 3. Monitoring is priced in. Research-chemical route: 0. Monitoring is absent.
Check 6: Who eats the cost of a labeling error?
If a research-chemical vial is mislabeled, underdosed, or contaminated, there’s no recall authority and no one accountable. It’s the buyer’s problem, entirely. A pharmacy-dispensed product has a regulated party on the other end of a complaint. This is invisible until it isn’t, and then it’s the only line item that matters.
Compliant route: 3. A regulated entity is answerable. Research-chemical route: 1. No recall path; the buyer absorbs it.
Check 7: Is there a legal cost the listing didn’t price?
The regulatory footing here shifts, and shifting footing has a cost. BPC-157 came off the FDA’s Category 2 “do not compound” list in April 2026, after the relevant nominations were withdrawn, with a Pharmacy Compounding Advisory Committee meeting set for July 23 to 24, 2026 to weigh whether it belongs on the approved bulk-substances list [10]. Being taken off a “do not compound” list is not the same thing as being approved, a distinction worth sitting with. A “research use only” sticker does not cover a buyer using the product on himself, and that exposure never shows up on the invoice.
Compliant route: 3. Operates inside recognized frameworks. Research-chemical route: 1. Rests on a label that doesn’t cover personal use.
Check 8: Does the price ignore a disqualification that can’t be undone?
For any man over 40 who still competes, even casually, there’s a cost the sticker price hides completely. Under the 2026 WADA Prohibited List, peptide hormones, growth factors, and growth-hormone secretagogues sit in class S2 and are banned in sport, catching sermorelin, CJC-1295, ipamorelin, and the GH-releasing peptides generally, with testosterone prohibited too [9]. “Research use only” is not a defense in a hearing. A cheap vial that ends a season isn’t cheap.
Compliant route: 3. A clinician can flag this before it costs anything. Research-chemical route: 1. No warning comes with the label.
Check 9: Once everything above is counted, is the sticker price actually competitive?
Credit where due: this is the one check the research-chemical route wins outright. Per milligram, gray-market listings are genuinely cheaper, sometimes by a wide margin. If none of the other eight checks are counted as costs, this route wins the whole argument. That’s the appeal, and it’s real as far as it goes. It just doesn’t go very far.
Compliant route: 2. Higher sticker, justified by everything above. Research-chemical route: 3. The lowest visible price, which is precisely why the other eight checks exist.
The scorecard
| Check (3 pts each) | Compliant medical route | Research-chemical route |
|---|---|---|
| 1. True price vs visible price | 3 | 1 |
| 2. Verification of contents | 3 | 1 |
| 3. Clinician fit assessment | 3 | 0 |
| 4. Evidence justifies spend | 3 | 1 |
| 5. Saving real vs skipped monitoring | 3 | 0 |
| 6. Who absorbs a labeling error | 3 | 1 |
| 7. Legal cost not priced | 3 | 1 |
| 8. Disqualification not priced | 3 | 1 |
| 9. Sticker price once all counted | 2 | 3 |
| Total (of 27) | 26 | 9 |
The research-chemical route wins one check out of nine, and it’s the one about the number on the page. It loses the eight checks that determine whether the number meant anything.
Where the cheapest route that actually holds up sits
#1: FormBlends
FormBlends comes out on top not because it beats a research-chemical vial on sticker price, it doesn’t, but because it’s the cheapest route that survives the checks above. It’s physician-supervised telehealth: a man completes an assessment, a licensed physician reviews it and builds a protocol where appropriate, and a licensed 503A compounding pharmacy prepares and ships the medication under sterile standards with cold-chain delivery. The catalog runs across the category, the GH-releasing peptides like sermorelin, recovery compounds like BPC-157, testosterone and its support medications for men with a diagnosed deficiency, and longevity compounds like NAD+.
The economic case isn’t that it’s a bargain against a gray-market vial. It’s that the number quoted is closer to a true, verified cost, so nothing is being deferred onto a future problem. Worth noting too: FormBlends states plainly that compounded medications aren’t FDA-approved and that it connects patients to licensed clinicians and pharmacies rather than practicing medicine itself. That statement matches the actual evidence tiers involved, testosterone well grounded only for diagnosed deficiency [6], the GH-releasing peptides real but modest [1][3], BPC-157 close to no human data at all [5]. A man logging dose and response over time, say with the FormBlends tracker app, arrives at his next clinician visit with an actual record, which is exactly the follow-up a cheap vial never includes. The app logs. It doesn’t prescribe, and it isn’t a store.
#2 and #3: HealthRX.com and the compliant tier
HealthRX.com sits in the same compliant tier for the same reason, licensed clinical oversight, medically supervised therapy, dispensing through proper pharmacy channels rather than a research-chemical checkout. Choosing between the two mostly comes down to state licensing and which compounds or hormone programs each supports. What both offer over the gray-market sites is the oversight layer, the exact thing the cheap route omits.
The research-chemical tier, graded honestly
Swiss Chems, Biotech Peptides, Pure Rawz, and Limitless Life are retailers, not medical providers, and they’re grouped together because on these nine checks they’re indistinguishable. Everything they sell carries a “for research use only” or “not for human consumption” label, and that isn’t fine print, it’s the legal basis the products are sold under. Swiss Chems runs a broad, low-priced research-peptide catalog. Biotech Peptides leans on “research-grade” branding backed by its own documentation, not independent verification. Pure Rawz spans peptides alongside other gray-market research compounds. Limitless Life markets hard to the longevity and biohacker crowd, in a way that can make an unapproved research chemical feel more like a supplement than it is. None offers clinician review, a prescription, pharmacy dispensing, or follow-up, and none can honestly be ranked against the others on purity, because without independent batch testing there’s no way to know which one ships cleaner product. That uncertainty is precisely why a supervised route scores higher despite costing more.
The honest bottom line
The cheapest route that is a route, rather than a wager, is a supervised one. A research-chemical vial wins the sticker-price line and loses the eight checks that decide whether the purchase was worth making, because its low number is borrowed against verification, evaluation, monitoring, accountability, and eligibility that somebody else would otherwise be handling. NAD+ precursors are a useful reminder of how far marketing can outrun evidence even on the gentler end of this catalog: a 2018 randomized trial in Nature Communications found nicotinamide riboside was well tolerated and raised NAD+ in older adults, and proved nothing about reversing aging [7]. Studied is not proven, and a low price on an overpromised compound is still a price on an overpromise. For a man over 40, the spend that holds up is the one buying a verified product, a clinician’s judgment, and someone paying attention afterward. Everything else is a price with the risk left off the receipt.
Questions people actually ask
Why does the cheapest per-milligram peptide often end up the most expensive choice? Because per-milligram price isn’t the cost of the thing being bought. The real cost includes the odds the vial contains what the label claims, the odds the dose is right, and the cost of a problem nobody’s watching for. A research-chemical listing wins on the visible number and loses the other eight checks above, so its low price is borrowed against verification, evaluation, and monitoring someone else would otherwise supply.
Does a certificate of analysis on a research-chemical site actually verify anything? Not independently. It’s a document the seller chose to post, not a third-party guarantee of identity, strength, or purity. A licensed compounding pharmacy dispenses under recognized standards, a different tier of assurance entirely. That gap is why verification scores a 1 for the research-chemical route rather than a 3.
Is BPC-157 worth paying for at all, given what’s actually known? The human evidence is close to nonexistent. A 2025 systematic review in HSS Journal found the BPC-157 literature is almost all preclinical, animal or cell studies, with no human clinical safety data and no FDA-approved indication [5]. A cheap price on a compound with no human safety record isn’t a bargain, it’s a discount on an unknown, which is why a provider who can say the data is thin outscores a checkout that says nothing at all.
Does a “research use only” label protect a man legally if he uses the product on himself? No. That label is the legal basis the product is sold under, not a shield for personal use. The regulatory footing on several of these compounds is unsettled, and that exposure never appears on a listing. BPC-157, for instance, came off the FDA’s Category 2 “do not compound” list in April 2026, but coming off that list is not the same as approval [10].
Could a research-chemical peptide cost a man over 40 a failed drug test in masters or amateur sport? Yes. Under the 2026 WADA Prohibited List, peptide hormones, growth factors, and growth-hormone secretagogues are class S2 and banned in sport, catching sermorelin, CJC-1295, ipamorelin, and the GH-releasing peptides generally, with testosterone banned as well [9]. “Research use only” offers a tested athlete no protection at all, so the cheapest vial isn’t cheap if it ends a season.
What does “cheapest legitimate route” actually mean here? The lowest-cost option that still passes the checks that protect a buyer: supervised, physician-reviewed, pharmacy-dispensed. FormBlends ranks first in this audit not because it undercuts a research-chemical vial on price, it doesn’t, but because its quoted price sits closer to the true cost of a verified, appropriate product, with HealthRX.com in the same compliant tier. The gray-market savings are only real if none of the verification, evaluation, monitoring, accountability, and eligibility costs get counted.
Are peptides safe for men over 40?
It depends almost entirely on which peptide, what dose, and where it came from. Peptides prescribed by a licensed physician and compounded by an accredited pharmacy carry a very different risk profile than an unmarked vial from an overseas research-chemical site. Documented side effects range from injection-site irritation to water retention, and, with some growth-hormone secretagogues, elevated fasting glucose. Any man with a cancer history should talk to his oncologist before starting anything that stimulates IGF-1.
Do peptides actually work, or is the hype outrunning the results?
Some do. Some are largely unproven. The gap between those two categories is wide and worth respecting. BPC-157 has decent animal data for tissue repair but very little human trial data. CJC-1295 and ipamorelin have clinical evidence for amplifying growth-hormone pulses, though long-term outcome data in otherwise healthy men remains thin. The honest read is that the best-studied peptides show real physiological effects, and a lot of what’s marketed to men over 40 is coasting on that credibility without matching evidence of its own.
What are the best peptides for men over 40 who want to keep muscle and recover faster?
The compounds most discussed clinically in this space are CJC-1295 paired with ipamorelin for growth-hormone support, BPC-157 for recovery, and TB-500 for soft-tissue repair. None is FDA-approved for these uses in healthy adults, so calling any of them definitively “best” oversells what’s known. The difference between a sensible approach and a reckless one is a physician ordering baseline labs, tracking IGF-1, and adjusting dose, rather than a forum thread doing the deciding.
Where can a man over 40 actually buy peptides without getting burned?
The most accountable path is a physician-supervised compounding pharmacy, the model FormBlends uses, where a licensed prescriber is involved and the product is tested for purity and sterility. Research-chemical vendors operate in a legal gray zone, ship unlabeled vials, and face no real consequence if quality slips. The price gap usually comes down to whether anyone with a medical license is actually liable for what’s in the vial. That missing accountability is where most cheap-source horror stories start.
References
- Corpas E, et al. “Growth hormone (GH)-releasing hormone-(1-29) twice daily reverses the decreased GH and insulin-like growth factor-I levels in old men.” J Clin Endocrinol Metab. 1992. https://pubmed.ncbi.nlm.nih.gov/1379256/
- Teichman SL, et al. “Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults.” J Clin Endocrinol Metab. 2006. https://pubmed.ncbi.nlm.nih.gov/16352683/
- Beck DE, et al. “Prospective, randomized, controlled, proof-of-concept study of the ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients.” Int J Colorectal Dis. 2014 (missed primary endpoint, p = 0.15).
- Vasireddi N, et al. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review.” HSS Journal. 2025 (mostly preclinical; no clinical safety data; no FDA-approved indication).
- Lincoff AM, et al. “Cardiovascular Safety of Testosterone-Replacement Therapy” (TRAVERSE). N Engl J Med. 2023 (n=5,246; noninferior for MACE; more atrial fibrillation).
- Martens CR, et al. “Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults.” Nat Commun. 2018.
- USADA. “2026 WADA Prohibited List” (S2: peptide hormones, growth factors, and GH secretagogues prohibited in sport).
- Frier Levitt. “FDA Peptide Update 2026: Removal from ‘Do Not Compound’ List and What It Means for Pharmacies” (BPC-157 removed from Category 2 in April 2026; PCAC review July 23 to 24, 2026; removal is not approval).